EXPANDER/ IMPLANT/ MATRIX
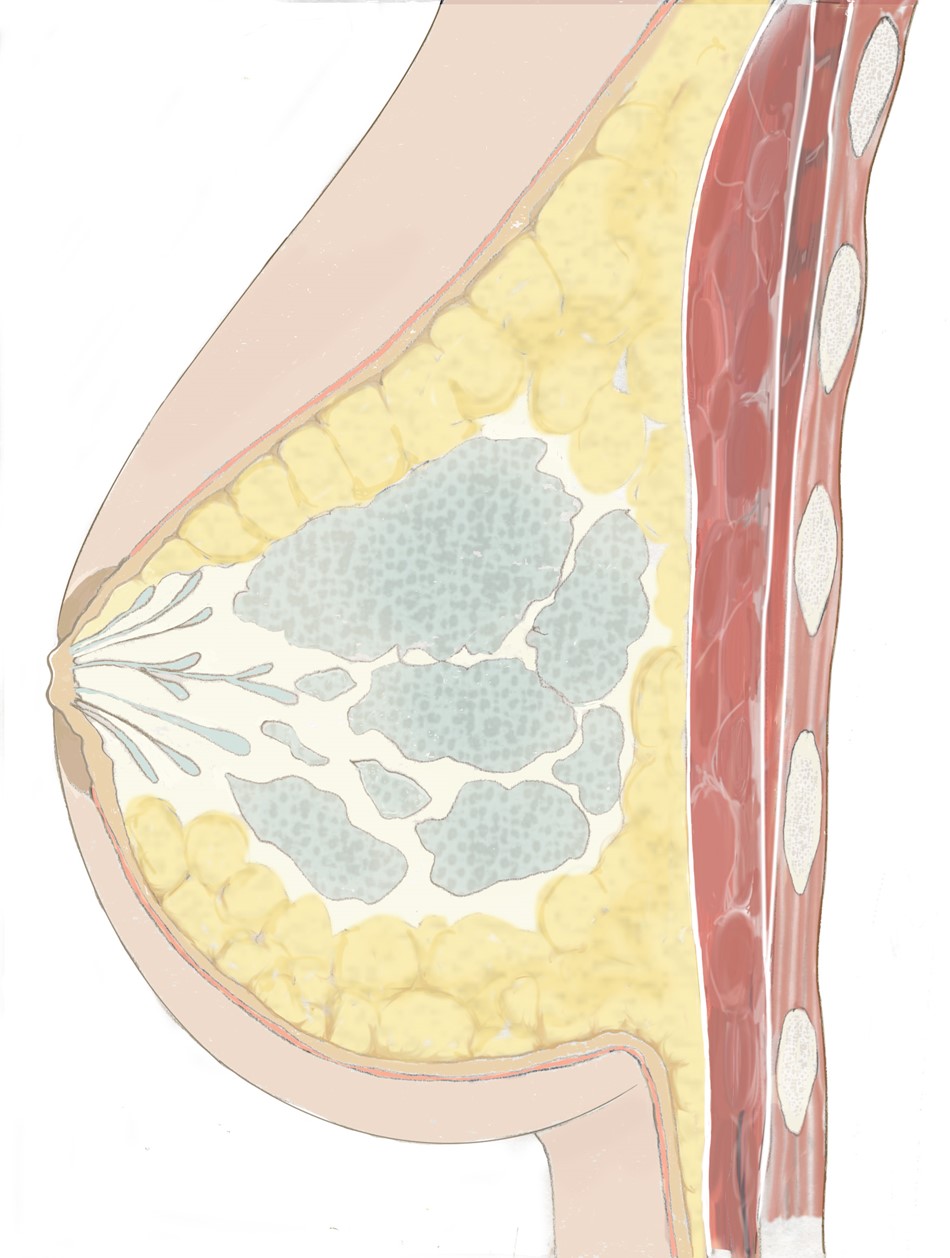
One option for replacing the missing breast tissue is to use a silicone implant. During the first stage, at the time of removal of the breast (mastectomy), a temporary implant, also known as a tissue expander, is inserted. The expander serves primarily as a place holder, allowing the breast skin to recover after the mastectomy.
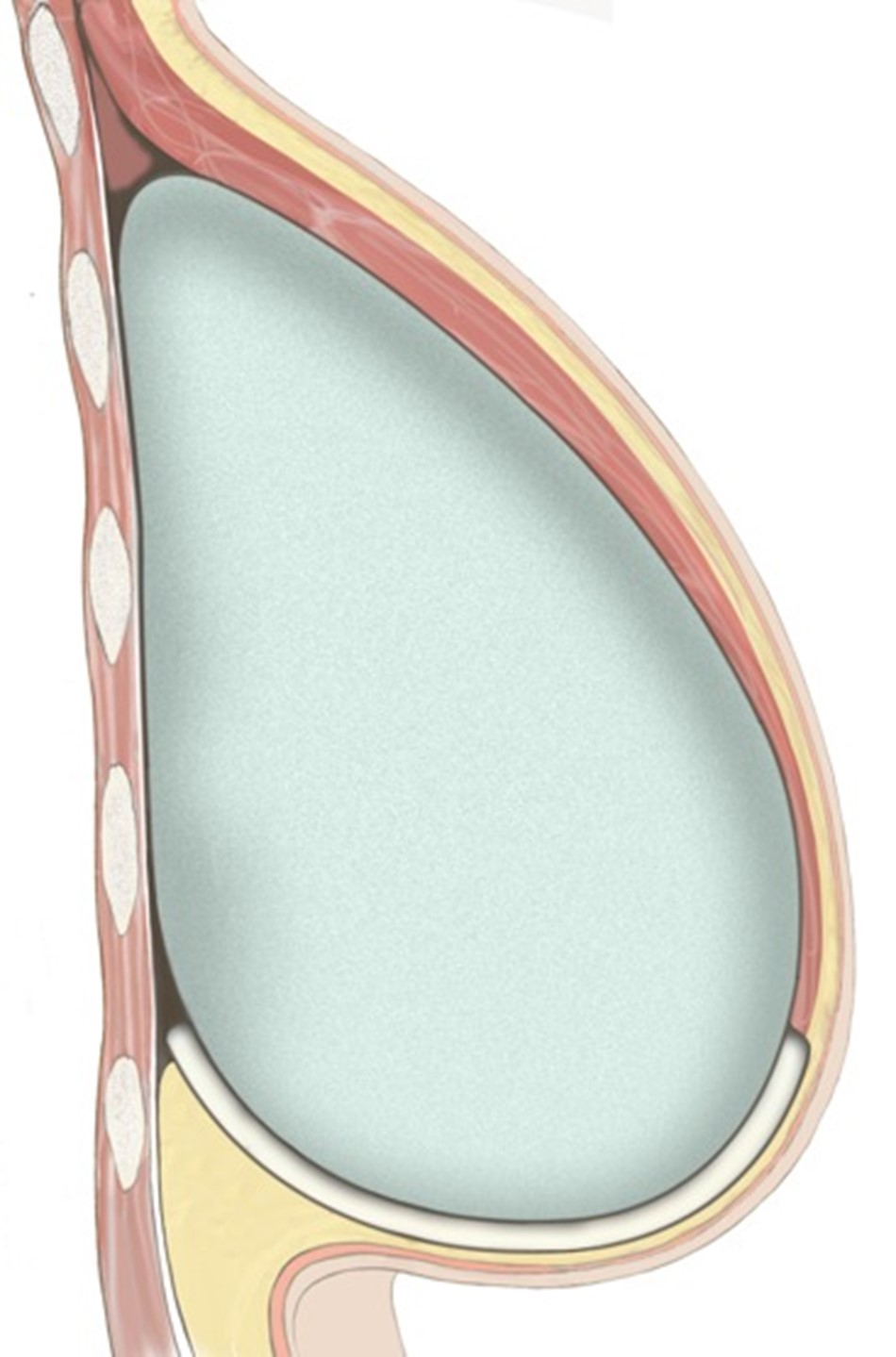
At a second stage, the definitive silicone implant is inserted. Under specific circumstances, the definitive implant may have already been used in the first operation. The implant is placed under the pectoralis muscle. However, as the pectoralis muscle only provides cover to the top half of the implant, an additional matrix is used to provide cover to the bottom half of the implant. The matrix also acts as a hammock, thereby supporting the implant and optimising the position to enhance the results of the reconstruction.